What Is Methylene Blue? The Oldest Synthetic Drug’s Second Life
A blue dye older than aspirin helped found the pharmaceutical industry and still treats a rare blood disorder. At low concentrations it is now studied as a mitochondrial “electron cycler” for the brain — with a sharply two-sided dose-response.
Methylene Blue (methylthioninium chloride) is a phenothiazine dye and an approved medicine for methemoglobinemia. At low concentrations it is studied preclinically as an alternative mitochondrial electron carrier proposed to support ATP production. It is not an approved cognitive enhancer anywhere; Condor supplies it strictly as a research-grade reference material, characterised for identity and purity and accompanied by a Certificate of Analysis — not for human or veterinary use.
In 1876, a young German chemist named Heinrich Caro pulled a vivid blue compound out of coal tar. It was meant to dye cotton. Within a decade it would stain bacteria under a microscope, be turned against a strain of malaria, and become — by most reckonings — the first fully synthetic drug ever given to a patient. That molecule, methylene blue, is older than aspirin. And in one of the strangest second acts in pharmacology, the same blue dye that helped found the entire pharmaceutical industry is now being studied as a kind of battery-booster for the mitochondria inside neurons3.
It is a story worth telling carefully, because methylene blue sits at an unusual intersection: a genuinely approved medicine, a workhorse laboratory reagent, and a compound that has attracted intense and often uncritical enthusiasm online. The science is real. So are the caveats. The interesting part is how tightly the two are bound together — in this molecule, the line between helpful and harmful is drawn almost entirely by concentration.
What exactly is methylene blue?
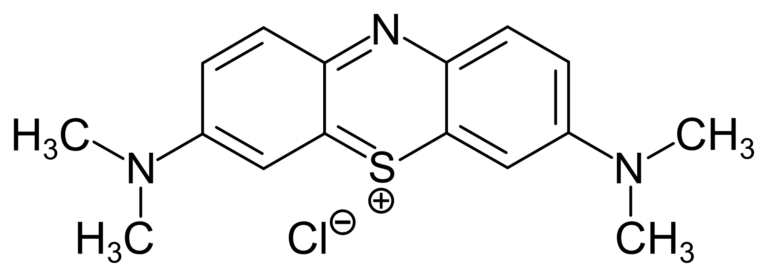
Chemically, methylene blue is methylthioninium chloride, a member of the phenothiazine family of dyes. It is an intensely coloured, water-soluble salt — so coloured that a few milligrams tint a litre of water a deep, unmistakable blue, and it will stain skin, tissue and urine the same shade with cheerful indifference. That visibility is not a side note; it is central to its history. Paul Ehrlich used it to selectively stain nerve tissue and microbes, an observation that seeded his entire “magic bullet” theory of targeted drugs3.
Today methylene blue has one clear, uncontested medical job: it is an approved treatment for methemoglobinemia, a condition in which haemoglobin loses its ability to carry oxygen3. It also serves as a diagnostic and surgical dye. Both uses turn on the same trick — the molecule’s willingness to gain and shed electrons. The material Condor supplies is research-grade reference material, characterised for identity and purity, and intended for research use only.
How does methylene blue affect mitochondria?
Here is where the second life begins. Mitochondria generate ATP by passing electrons down a chain of protein complexes — the electron transport chain — until they reach cytochrome-c-oxidase, which hands them to oxygen. Think of it as a bucket-brigade passing energy from hand to hand. When one of the hands falters, the whole line backs up.
At low concentrations, methylene blue is proposed to slip into that brigade as an alternative electron carrier314. It accepts electrons upstream and delivers them further down the chain, effectively rerouting around bottlenecks and, in preclinical models, supporting cytochrome-c-oxidase activity and ATP output315. In the same low-concentration window it has been reported to scavenge reactive oxygen species, behaving as an antioxidant38. Because the brain is one of the most energy-hungry and mitochondria-dense tissues in the body, this electron-cycling behaviour is precisely why methylene blue became a candidate for neuroprotection and cognition research.
But — and this is the whole story in one word — the effect is hormetic. The very redox chemistry that helps at low concentrations reverses at higher ones, where methylene blue stops donating electrons usefully and starts generating oxidative stress instead53.
Methylene blue is widely regarded as the first fully synthetic drug used in medicine — in clinical and laboratory use since the late nineteenth century, older than aspirin, and still an approved treatment for methemoglobinemia today.
What has the research actually shown?
The preclinical breadth is genuinely striking. In rodent and cell models, low-concentration methylene blue has been studied across a range of energy-failure conditions: traumatic brain injury, cerebral ischaemia, and optic-nerve injury models, where mitochondrial support appears protective3911. It has been examined against mitochondrial dysfunction and ageing-related endpoints15. In the clinic, it has been explored for perioperative neurocognitive disorders — the cognitive fog that can follow surgery and anaesthesia — though that early human work remains limited and preliminary1.
The most ambitious chapter has been Alzheimer’s disease. Methylene blue inhibits the aggregation of tau, the protein that tangles inside neurons in Alzheimer’s, which made it a logical candidate3613. This led to randomised trials of methylene-blue derivatives designed to be more stable and better absorbed6. The candour required here is essential, and it leads directly into the part of this molecule’s story that the enthusiasm tends to skip.
| Attribute | What it is | The caveat |
|---|---|---|
| Approved use | Methemoglobinemia (and a diagnostic/surgical dye) | NOT approved as a nootropic or cognitive enhancer anywhere |
| Low-concentration mechanism | Proposed alternative mitochondrial electron carrier; supports ATP, mild antioxidant in models | Hormetic — the same chemistry turns pro-oxidant at higher concentrations |
| Dose-response shape | U-shaped: helpful at low concentrations | Pro-oxidant and toxic at higher ones, where it behaves as a penetrating cation |
| Pharmacology flag | Potent monoamine-oxidase inhibitor (MAOI) | Serotonin-syndrome risk if combined with serotonergic drugs |
Methylene blue at a glance: a single molecule whose benefits and hazards are both governed by concentration and context.
What are the honest caveats about methylene blue?
Three things need stating plainly, because they are the difference between informed research and wishful thinking.
First, the U-shaped dose-response is not a footnote — it is the defining feature. The window in which methylene blue supports mitochondria is narrow, and above it the molecule behaves as a penetrating cation with genuinely toxic effects5. A compound whose helpful and harmful behaviours are produced by the same mechanism, separated only by concentration, demands far more respect than its reputation as a cheap blue powder suggests.
Second, methylene blue is a potent monoamine-oxidase inhibitor8. MAO inhibition is exactly how some older psychiatric drugs work, and it is also how serotonin can accumulate to dangerous levels. Combined with serotonergic medicines, methylene blue carries a recognised risk of serotonin syndrome8 — a serious reason it is never a casual substance, and one of the most consequential real-world hazards anyone handling the compound must understand.
Third, the clinical track record is sobering. Despite the elegant tau biology, trials of methylene-blue derivatives for Alzheimer’s have been largely disappointing6. The preclinical literature is broad and encouraging; the human evidence for cognition is far thinner and, where rigorously tested, often underwhelming63. That gap between rodent promise and human proof is the most important thing to carry away — and it is a theme that runs through the wider field of non-peptide nootropics, where compounds such as the curcumin-derived J-147 share the same mitochondrial logic and the same need for honest, preclinical-first framing.
Is methylene blue an approved nootropic?
No. This is the bottom line, and it should be unambiguous. Methylene blue is approved only for methemoglobinemia and as a diagnostic dye. It is not approved as a cognitive enhancer or nootropic in the EU, the US, or anywhere else. The mitochondrial cognition story is a research story — vivid, mechanistically plausible, and genuinely interesting — but it remains preclinical and early-clinical, not established human efficacy.
That is exactly why purity and provenance matter so much for this molecule. When a compound’s working window is defined by concentration, you cannot reason about it at all unless you know precisely what you have. A material of uncertain grade or unknown impurity profile is not a research tool; it is a guess. Condor supplies methylene blue as a research-grade reference material, characterised for identity and purity and accompanied by a Certificate of Analysis — not for human or veterinary use, and not as a cognitive enhancer. For a molecule this old, this useful, and this two-sided, knowing exactly what is in the vial is not a nicety. It is the entire premise of doing the science properly.
- Methylene Blue (methylthioninium chloride) was essentially the first fully synthetic drug, and it remains an approved treatment for methemoglobinemia and a diagnostic dye.
- At low concentrations it is proposed to act as an alternative mitochondrial electron carrier, shuttling electrons to support cytochrome-c-oxidase activity and ATP production — a hormetic effect that reverses at higher concentrations.
- It has been studied preclinically and in early clinical work for perioperative neurocognitive disorders, Alzheimer's-type pathology, traumatic brain injury, ischaemia and optic-nerve models — with results that remain far thinner in humans than in rodents.
- Two serious caveats: the dose-response is U-shaped (helpful low, pro-oxidant and toxic high), and it is a potent monoamine-oxidase inhibitor carrying serotonin-syndrome risk with serotonergic drugs.
- It is approved ONLY for methemoglobinemia, NOT as a nootropic anywhere; Condor supplies research-grade material for research use only, characterised for identity and purity with a Certificate of Analysis — not for human or veterinary use.
Is methylene blue safe to take as a nootropic?
Methylene blue is not approved as a nootropic anywhere and should not be treated as a consumer product. Its dose-response is U-shaped — helpful at low concentrations in research models but pro-oxidant and toxic at higher ones — and it is a potent monoamine-oxidase inhibitor that can cause serotonin syndrome when combined with serotonergic drugs. Condor supplies it for research use only, not for human or veterinary use.
What is methylene blue actually approved for?
Methylene blue (methylthioninium chloride) is an approved medicine for methemoglobinemia, a blood disorder in which haemoglobin cannot carry oxygen properly, and it is also used as a diagnostic and surgical dye. Its use in cognition and neuroprotection research is preclinical and early-clinical, not an approved indication.
How does methylene blue affect the mitochondria?
At low concentrations, methylene blue is proposed to act as an alternative electron carrier in the mitochondrial electron transport chain, accepting and donating electrons to support cytochrome-c-oxidase activity and ATP production, with mild antioxidant behaviour reported in models. This effect is hormetic and reverses at higher concentrations, where the same redox chemistry becomes pro-oxidant and toxic.
Why is the dose-response of methylene blue described as U-shaped?
Because the molecule's benefits and harms come from the same redox chemistry, separated only by concentration. Low concentrations are reported to support mitochondrial energy production and act as a mild antioxidant; higher concentrations make it a pro-oxidant penetrating cation with toxic effects. The useful window is narrow, which is why concentration and purity are critical in any research setting. It is also a potent monoamine-oxidase inhibitor, adding serotonin-syndrome risk alongside serotonergic drugs.
Did methylene blue work for Alzheimer's disease?
Methylene blue inhibits aggregation of the tau protein, which made it a logical Alzheimer's candidate, and randomised trials of methylene-blue derivatives were conducted. Despite strong preclinical rationale, the human results have been largely disappointing — a clear example of the gap between rodent-model promise and proven human efficacy.