KPV vs Larazotide: Two Peptides in Gut-Barrier and Inflammation Research
KPV and larazotide are both studied in intestinal-barrier and inflammation research, but by different mechanisms. A sober, RUO comparison — including larazotide's negative phase III result. References verified.
KPV and larazotide are two distinct peptides studied in intestinal-barrier and inflammation research, and they are not interchangeable. KPV is the C-terminal tripeptide of alpha-MSH (Lys-Pro-Val), studied preclinically as an anti-inflammatory fragment taken up by intestinal cells through the PepT1 transporter. Larazotide (AT-1001) is an eight-amino-acid tight-junction regulator that antagonises the zonulin/PAR2 pathway to reduce paracellular permeability. The mechanisms differ — KPV dampens inflammatory signalling inside the cell, larazotide acts on the junctions between cells. Crucially, larazotide is the more clinically advanced of the two but reached phase III in coeliac disease and the programme was discontinued for futility; KPV has no human clinical trials at all. Both are research-use-only reference materials, not medicines, and neither is approved for any "leaky gut" indication.
Two peptides keep surfacing in the same conversations about the intestinal barrier, and they are almost always conflated. KPV and larazotide both turn up in discussions of inflammation, permeability and the fashionable, ill-defined idea of a “leaky gut.” But they are different molecules doing different things — one works inside the cell, the other works on the seams between cells — and their evidence sits at very different altitudes. One of them, larazotide, did the rare and honourable thing of walking into a large late-stage clinical trial. What happened there is the most important part of this comparison, and the part most often left out.
Both are sold strictly for research use only (RUO), as laboratory reference materials for in-vitro and animal-model investigation of intestinal-barrier biology and inflammatory signalling. What follows is a sober reading of what the verifiable literature actually shows — and where it stops. No dosing, no administration guidance, no therapeutic claims of any kind.
What are KPV and larazotide, chemically?
KPV is the tripeptide Lys-Pro-Val — the carboxy-terminal sequence (residues 11–13) of alpha-melanocyte-stimulating hormone (alpha-MSH), a 13-residue hormone derived from pro-opiomelanocortin. For decades, investigators asked which part of alpha-MSH carries its quieter, anti-inflammatory reputation; the answer pointed repeatedly to the tail. KPV is the minimal fragment isolated to test that idea directly, and its appeal is precisely its smallness — a defined three-residue sequence that is cheap to synthesise and chemically tractable.7 You can read the full primer in our KPV explainer.
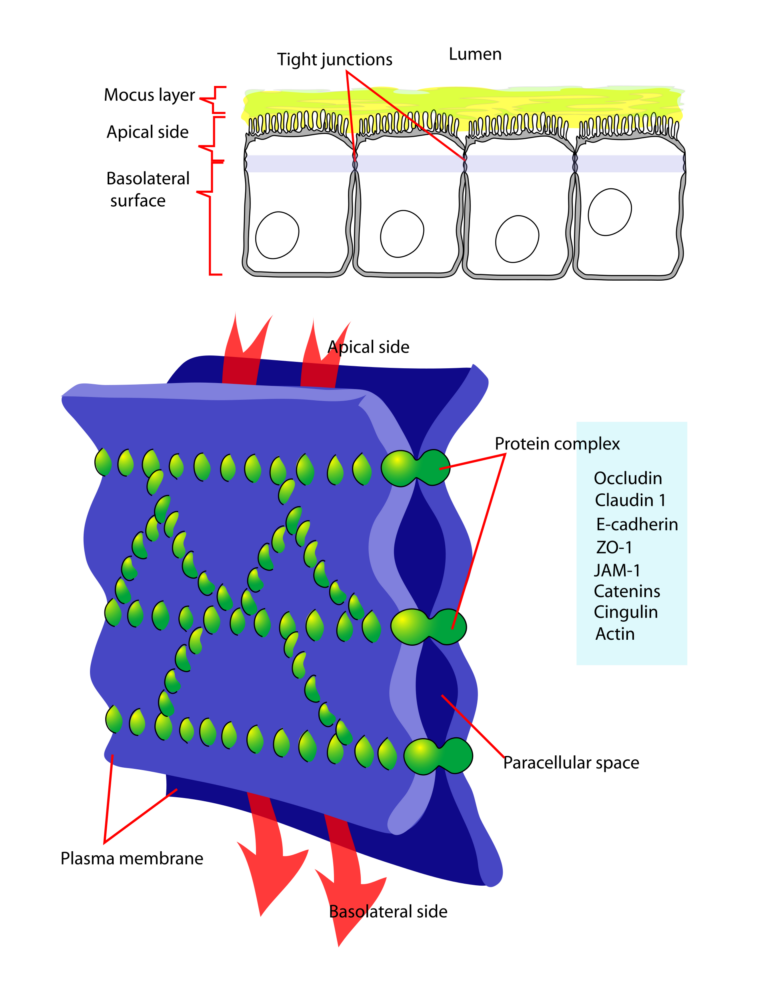
Larazotide, catalogued as AT-1001, is a synthetic eight-amino-acid peptide engineered for a single, narrow job: holding the seams of the intestinal lining shut. The gut lining is one cell thick, and the spaces between those cells are stitched closed by protein zippers called tight junctions. Larazotide was designed as a deliberately minimal, gut-restricted peptide that acts locally on those junctions rather than circulating through the body.9 The full background lives in our larazotide primer.
The chemistry already tells you they are not siblings. KPV is a fragment of a natural hormone; larazotide is a purpose-built synthetic peptide more than twice its length. The only thing they truly share is a research neighbourhood.
How do the two products compare?
| Attribute | KPV | Larazotide |
|---|---|---|
| Identity | Lys-Pro-Val (Lys-Pro-Val) | Larazotide acetate (AT-1001) |
| Origin | C-terminal fragment of alpha-MSH (residues 11–13) | Synthetic, rationally designed peptide |
| Length | 3 amino acid residues | 8 amino acid residues |
| Where it acts | Inside intestinal epithelial cells (via PepT1 uptake) | Between cells, at the tight junctions |
| Mechanism studied (preclinical) | NF-κB / MAPK inhibition; IL-1 antagonism; PepT1 transport | Tight-junction stabilisation; zonulin / PAR2 antagonism; lower paracellular permeability |
| Most advanced human data | None — preclinical only (cell & animal models) | Phase III in coeliac disease — discontinued for futility |
| Format supplied | Vial (also available as capsules) | Capsules |
| Purity / QC | ≥99% HPLC, MS-confirmed, COA, independent EU lab | ≥99% HPLC, MS-confirmed, COA, independent EU lab |
| Also available as | KPV Capsules | — |
Side-by-side framing of the two peptides as supplied by Condor Research. Note the asymmetry that matters most: larazotide is the more clinically tested compound, yet its pivotal trial was negative; KPV has no human trials at all. Both are research-use-only reference materials.
What does the research explore for KPV?
KPV’s literature is an inside-the-cell story. One of its most cited findings concerns how the tripeptide even gets in: in dextran-sulphate-sodium (DSS) and trinitrobenzene-sulphonic-acid (TNBS) colitis models used to mimic inflammatory bowel disease in mice, KPV is taken up by intestinal epithelial cells through PepT1, the di- and tri-peptide transporter that normally absorbs the products of protein digestion. That PepT1-mediated uptake was associated with reduced intestinal inflammation in those models.1 A separate study in murine IBD models reported anti-inflammatory potential for the melanocortin-derived tripeptide along the same lines.2
Once inside, KPV appears to touch the master switches of the inflammatory programme — the kind of work attributed to alpha-MSH-related peptides describes interference with NF-κB signalling and the IL-1 pathway in immune and epithelial systems.7 Beyond inflammation, the C-terminal melanocortin peptides have a documented antimicrobial streak,5 and the candidacidal chemistry of a KPV-containing construct has been characterised structurally.6 The translational interest is real enough that researchers have built delivery vehicles for it: orally targeted, hyaluronic-acid-functionalised nanoparticles carrying KPV alleviated ulcerative colitis in a mouse model,4 and the PepT1 route has been probed in colitis-associated cancer models too.3
3 KPV is just three amino acid residues — Lys-Pro-Val — reproducing several anti-inflammatory activities of a 13-residue hormone in a fraction of the size. Every finding here is preclinical: cell culture and animal models, not human outcomes.
What does the research explore for larazotide?
Larazotide’s story is the opposite geometry — it works on the spaces between cells. Mechanistic work shows it promotes tight-junction assembly in epithelial cells, redistributing junctional proteins toward a more sealed state,9 and reviews position it as a counterweight to zonulin, the endogenous regulator of tight-junction tone whose dysregulation has been linked to a leakier barrier in inflammatory disease.8 In a porcine model, larazotide promoted recovery of ischemia-injured jejunum specifically through repair of tight junctions.11
Unlike KPV, larazotide carries genuine human trial data. In a randomised, double-blind trial of adults with coeliac disease and persistent symptoms despite a gluten-free diet, the lowest dose was associated with fewer gastrointestinal symptoms than placebo10 — and an earlier gluten-challenge study examined whether tightening the barrier blunted the gut’s response to deliberate gluten exposure.12 Larazotide became the most advanced candidate in a field long promising options beyond the diet, and the standing example in reviews of emerging coeliac therapeutics.13
“Larazotide reached phase III in coeliac disease and the programme was discontinued for futility. That is not a footnote to bury — it is the most important fact in this comparison.”
And here candour has to override salesmanship. Larazotide advanced to phase III — the large, late-stage trial that decides whether a candidate becomes a medicine — and the programme was discontinued after an interim analysis concluded the study could not realistically reach its primary endpoint.13 The barrier mechanism is elegant; the clinical readout, at the scale that counts, was not positive. A futility stop does not mean the molecule is inert or the biology is fiction — it means the clean translational story did not hold the way its proponents hoped. Since then, larazotide has reappeared only in more exploratory settings, including a small phase 2a study and a case series in children with post-COVID multisystem inflammatory syndrome (MIS-C), where treatment was associated with faster clearance of viral spike antigen.1516 Intriguing, all of it — and all of it firmly upstream of approved clinical use.
KPV vs larazotide: which mechanism for which question?
There is no potency ranking here, only a question of what you are trying to model. The two peptides interrogate intestinal-barrier biology from opposite sides of the cell membrane, which is precisely why a thorough programme might use both.
Investigators probing intracellular inflammatory signalling — NF-κB and MAPK dynamics, IL-1 antagonism, PepT1-dependent uptake into epithelium — typically reach for KPV, the well-defined minimal fragment with a coherent preclinical literature.12 Those studying the physical barrier itself — tight-junction assembly, paracellular permeability, the zonulin/PAR2 axis — turn to larazotide, the most mechanistically characterised tight-junction regulator in the field, with the unusual distinction of an actual (if negative) late-stage clinical record.913 The honest comparison is not “which is better” but “which boundary are you studying — the cell’s interior, or the seal between cells?” For the broader landscape of these and related compounds, see our overview of leaky gut, zonulin and larazotide.
Preclinical or clinical — where does the evidence actually sit?
This is the distinction that should calibrate every claim. KPV sits entirely in the preclinical domain — cell culture and animal models, chiefly mice, with no human clinical trials establishing efficacy or safety for any condition.13 Larazotide reached the clinic and went further than almost any peptide in this space, but its pivotal phase III programme was halted for futility, and its newer findings are early, often single-group, and exploratory.1316 Neither compound is established as safe or effective in humans; neither is a drug, supplement, or treatment for any intestinal-barrier indication; and “leaky gut” as a catch-all diagnosis is not clinically recognised. Honest evidence means letting the negative result sit beside the promising mechanism rather than quietly dropping it.
Both Condor Research materials are supplied at ≥99% HPLC purity, identity-confirmed by mass spectrometry, with a per-batch Certificate of Analysis from an independent EU laboratory in Czechia, and both are intended exclusively for qualified research professionals. For laboratory research use only (RUO). Not for human or veterinary use, ingestion, or diagnostic application. No therapeutic claims are made or implied.
Research use only (RUO). The peptides discussed here are laboratory reference materials, not medicines, supplements, or treatments. They are not approved for human or veterinary use, and nothing in this article is a dose, protocol, or therapeutic recommendation. Published human studies are summarised strictly as reported science.
Condor Research · Scientific desk
- KPV (Lys-Pro-Val) is the C-terminal tripeptide of alpha-MSH; larazotide (AT-1001) is a synthetic eight-residue peptide — different molecules, different mechanisms.
- KPV is studied as an intracellular anti-inflammatory fragment, entering intestinal epithelial cells via the PepT1 transporter and dampening NF-kB/MAPK signalling in preclinical models.
- Larazotide acts between cells, stabilising tight junctions and antagonising the zonulin/PAR2 pathway to lower paracellular permeability.
- Larazotide is the more clinically advanced peptide but its phase III coeliac-disease programme was discontinued for futility — the single most important fact in this comparison.
- KPV has no human clinical trials; all of its barrier and anti-inflammatory data come from cell and animal models.
- Both are research-use-only (RUO) reference materials, supplied at high purity with a Certificate of Analysis, and neither is a medicine or approved for any "leaky gut" use.
Are KPV and larazotide the same kind of peptide?
No. They share a research context — intestinal barrier and inflammation — but they are chemically and mechanistically distinct. KPV is the three-residue C-terminal fragment of alpha-MSH (Lys-Pro-Val), studied as an intracellular anti-inflammatory peptide. Larazotide is a synthetic eight-amino-acid peptide (AT-1001) designed to stabilise the tight junctions between cells. One acts inside the cell, the other on the spaces between cells.
Which has stronger evidence, KPV or larazotide?
It depends on what you mean by “stronger.” Larazotide is far more clinically advanced — it ran randomised human trials and reached phase III — but that programme was discontinued for futility, meaning the largest test did not show the expected benefit. KPV has a coherent preclinical story across cell and animal models but no human trials at all. Neither has a positive late-stage clinical result, and anyone selling either as a proven gut therapy is overstating the science.
Did larazotide work in clinical trials?
Early and mid-stage signals were encouraging — an earlier randomised trial in coeliac patients with persistent symptoms despite a gluten-free diet associated the lowest dose with fewer gastrointestinal symptoms than placebo. But the pivotal phase III programme in coeliac disease was discontinued after an interim analysis concluded it could not realistically meet its primary endpoint. That negative result is the load-bearing fact, not a footnote.
Can KPV or larazotide treat “leaky gut”?
No. “Leaky gut” is not a clinically recognised diagnosis, and neither peptide is an approved treatment for any intestinal-barrier indication. Both are sold strictly as research-use-only reference materials for laboratory and animal-model work. Nothing here is a dose, protocol, or therapeutic recommendation for humans or animals.
Why would a lab study both peptides together?
Because they probe the same biology from opposite directions. A barrier-research programme might use larazotide to interrogate tight-junction tone and the zonulin/PAR2 axis, and KPV to interrogate intracellular inflammatory signalling via PepT1 uptake. Running both lets investigators separate “junction” effects from “signalling” effects in the same model system.