What Is Larazotide? The One “Leaky Gut” Peptide That Reached a Phase III Trial
Larazotide (AT-1001) is an eight-amino-acid peptide designed to tighten the gut's molecular seams by antagonising the zonulin pathway. It is the only “leaky gut” molecule with a serious clinical dossier — and its largest trial is also the most honest thing about it.
Larazotide is an eight-amino-acid peptide studied as a tight-junction regulator that antagonises the zonulin/PAR2 pathway to reduce intestinal permeability. It is the most clinically advanced “leaky gut” candidate, having reached a phase III coeliac-disease trial. It is not an approved medicine for any use; Condor supplies it strictly as a research-use-only reference material with a Certificate of Analysis.
“Leaky gut” is one of those phrases that has escaped the laboratory and gone feral. It turns up in wellness podcasts, supplement adverts and the comment sections of every diet forum, usually unaccompanied by anything resembling a molecule. Which makes the story of larazotide unusual, even a little subversive: here is a real eight-amino-acid peptide, with a real proposed mechanism, that did the one thing almost nothing in the leaky-gut universe has ever done. It walked into a large, controlled, late-stage clinical trial. What happened next is the most interesting — and most honest — thing about it.
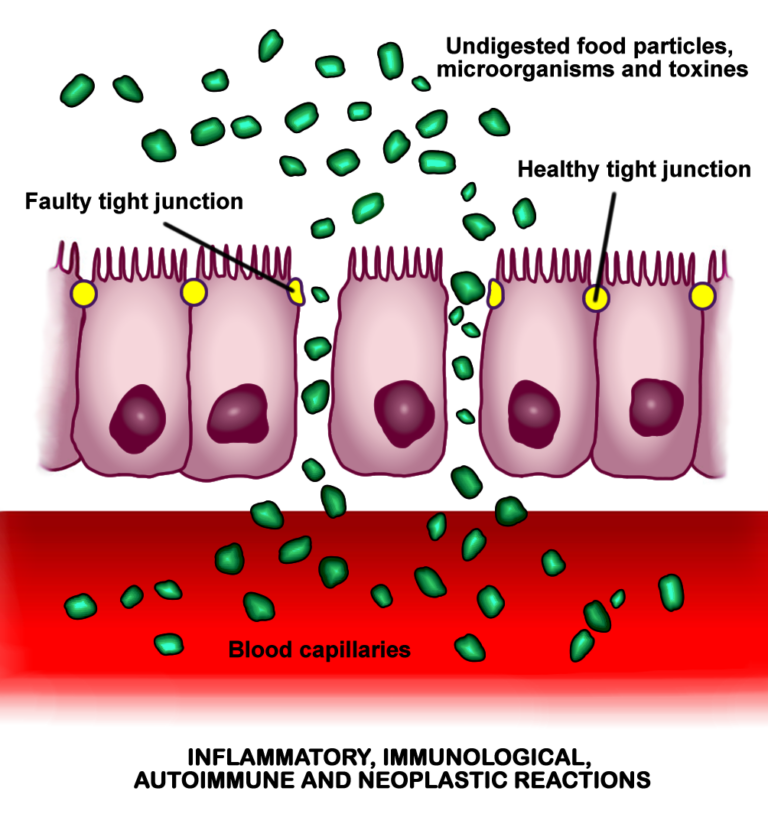
Larazotide, also catalogued as AT-1001, was conceived not as a cure for a fashionable syndrome but as a precise piece of barrier engineering. The intestinal lining is a single layer of cells, and the spaces between those cells are stitched shut by protein zippers called tight junctions.1 When the stitching loosens, the barrier becomes more permeable, and material that should stay in the gut lumen can cross into tissue underneath.2 In coeliac disease, that loosening is part of the problem: gluten fragments help pry the junctions open, and the immune system meets antigens it was never meant to see.5 Larazotide was designed to hold the zippers shut.1
How does larazotide actually work in the gut?
The mechanism hinges on a signalling molecule called zonulin, described as the body’s own physiological regulator of tight-junction tone.5 Think of zonulin as a doorman with a master key: when it is released, the junctions between cells relax and the barrier becomes more open. In chronic inflammatory disorders, several lines of evidence link elevated zonulin signalling to a dysregulated, leakier barrier.2 Larazotide is positioned as the counterweight — a tight-junction regulator that opposes this opening and nudges the barrier back toward a sealed state, an effect linked in mechanistic work to redistribution of tight-junction proteins and inhibition of myosin light-chain kinase.1
More recent pharmacology has sharpened the picture. Work on epithelial barriers describes larazotide as a PAR2 antagonist — blocking protease-activated receptor 2, a receptor whose activation drives barrier disruption.13 In keratinocyte models of skin inflammation, larazotide blunted histamine-stimulated barrier breakdown through exactly this PAR2 route, increasing transepithelial resistance and lowering permeability.13 Separate experiments show it protecting the intestinal mucosal barrier against anoxia-reoxygenation injury, preserving tight-junction organisation through several overlapping cellular mechanisms.14 Compared with much of the “gut peptide” field, this is a relatively well-characterised molecular story: a defined target, a plausible pathway, and a coherent reason to expect lower permeability.1
Larazotide is just eight amino acids long — a deliberately minimal, gut-restricted peptide engineered to act locally on tight junctions rather than circulate through the body.1
What happened in the coeliac-disease trials?
Coeliac disease was the obvious proving ground. For people with the condition, the only established management is lifelong, total avoidance of gluten — an exhausting, never-fully-achievable discipline, and one that leaves patients with no pharmacological backstop when contamination inevitably happens.4 A molecule that could blunt the gut’s response to incidental gluten would be genuinely useful in research terms, and larazotide became the most advanced candidate in a field that has long promised options beyond the diet.3
Across its development, larazotide was tested in coeliac patients deliberately re-exposed to gluten, the cleanest way to ask whether tightening the barrier translates into fewer symptoms.6 In one randomised, double-blind trial of 342 adults with persistent symptoms despite a gluten-free diet, the lowest dose was associated with fewer gastrointestinal symptoms than placebo — an encouraging signal that helped carry the molecule forward.6 It became the headline example in reviews of emerging coeliac therapeutics and the standing answer to the question of whether there might one day be a research path beyond gluten restriction.4 It also features prominently in surveys of new gastroenterology, where the appetite for non-dietary options is especially acute.3
And here is where candour matters more than salesmanship. Larazotide reached phase III — the large, late-stage trial that decides whether a drug becomes a medicine — and the programme was discontinued after an interim analysis concluded the study could not realistically meet its primary endpoint.3 The barrier story is elegant; the clinical readout, at the scale that counts, was not positive. Anyone selling larazotide as a proven gut therapy is either uninformed or hoping you are.
Where else is larazotide being studied?
A failed primary endpoint in one indication does not retire a molecule, and researchers have pushed larazotide’s barrier logic into several other settings — all of them earlier, and all of them more speculative than coeliac disease. The most striking is paediatric: a 2025 Science Translational Medicine study examined larazotide in children with post-COVID multisystem inflammatory syndrome (MIS-C), a small phase 2a trial reporting faster clearance of viral spike antigen and faster return to usual activities in the treated group.12 The hypothesis is that a leakier gut lets viral antigen persist, and that resealing the barrier helps the body clear it — an idea that remains exactly that, a single-study hypothesis.12
In animal and bench models the catalogue grows. Larazotide reduced markers of intestinal permeability in a preclinical NASH/non-alcoholic fatty liver model, consistent with a gut-liver axis in which a leakier barrier feeds hepatic stress.8 Bioengineers have loaded it into an antibacterial hyaluronic-acid hydrogel for sustained local release as an experimental colitis treatment in mice.11 And the dermatology work extends the same tight-junction principle to the skin barrier in atopic-dermatitis models.13 The connecting thread — that intestinal permeability is a lever worth pulling in inflammatory disease — remains an active, legitimate research question.2
| Research peptide | Primary mechanism studied | Evidence stage |
|---|---|---|
| Larazotide (AT-1001) | Tight-junction regulator; zonulin / PAR2 antagonist lowering permeability | Reached phase III in coeliac disease (programme discontinued, primary endpoint not met); other uses preclinical |
| KPV | Tripeptide studied for anti-inflammatory signalling in the gut and beyond | Preclinical / in vitro and animal models |
| BPC-157 | Gastric-derived peptide studied for tissue and mucosal repair | Preclinical; predominantly animal-model data |
Three peptides that recur in gut-barrier research, ranked by how far each has travelled toward the clinic. Larazotide is, by some distance, the most clinically tested — which is precisely why its negative phase III result is so informative.
What does the honest evidence say?
Strip away the marketing and a clear, defensible picture remains. Larazotide’s mechanism is comparatively well characterised: a defined peptide acting on a defined pathway (zonulin/PAR2 tight-junction regulation) to reduce intestinal permeability, supported by barrier and receptor studies.151314 That is more than can be said for most molecules in the leaky-gut conversation, and it is a real point in larazotide’s favour.
But mechanism is a hypothesis, not a verdict. The verdict, in coeliac disease, was a phase III programme stopped at interim analysis for inability to reach its primary endpoint — the most rigorous test larazotide has faced, and the one it did not pass.3 That outcome does not falsify tight-junction biology; barriers do loosen, zonulin signalling is real, and resealing them is a coherent goal.1 It does mean that translating clean mechanism into clinical benefit proved harder than the model predicted.6 The newer indications — MIS-C, NAFLD, colitis, dermatitis — are genuinely interesting but sit far earlier on the evidence ladder, mostly in single studies, animal models, or small exploratory cohorts.81112 Treating any of them as established would repeat the very over-reach the coeliac result should teach us to avoid. The same restraint applies to the broader literature on permeability and barrier function, which remains a moving research target rather than a settled clinical playbook.29 For a fuller treatment of where the zonulin model holds and where it frays, see our editorial on leaky gut, zonulin and larazotide.
Why does research-grade material matter here?
Larazotide is not an approved medicine for any indication, in the EU or anywhere else, and nothing on this page is dosing, protocol, or therapeutic advice for humans or animals. Condor supplies it strictly as a research-use-only reference material — an input for in vitro and animal-model work conducted by qualified researchers, not a product for consumption.
In that context, the unglamorous details are the ones that decide whether an experiment means anything. A peptide this short is defined entirely by its sequence and purity: a wrong residue, a truncated chain, or an undeclared contaminant turns a barrier study into noise.1 That is why every batch ships with a Certificate of Analysis documenting identity and purity. If you are not yet fluent in reading one, our guide on how to read a Certificate of Analysis is the place to start — because in tight-junction research, as in the larazotide story itself, the honest answer is always in the data.
References
- Slifer ZM, Krishnan BR, Madan J, Blikslager AT. Larazotide acetate: a pharmacological peptide approach to tight junction regulation. Am J Physiol Gastrointest Liver Physiol. 2021;320(6):G983–G989. PMID: 33881350.
- Sturgeon C, Fasano A. Zonulin, a regulator of epithelial and endothelial barrier functions, and its involvement in chronic inflammatory diseases. Tissue Barriers. 2016;4(4):e1251384. DOI: 10.1080/21688370.2016.1251384.
- Beyond the gluten-free diet: innovations in coeliac disease therapeutics. World J Gastroenterol. 2024;30(38):4194–4210. (Review of emerging non-dietary therapies, including the discontinued larazotide phase III/CeDLara programme.)
- Cardoso-Silva D, et al. New insights into non-dietary treatment in coeliac disease: emerging therapeutic options. 2021. PMC8308370.
- Fasano A. Zonulin and its regulation of intestinal barrier function: the biological door to inflammation, autoimmunity, and cancer. Physiol Rev. 2011;91(1):151–175. DOI: 10.1152/physrev.00003.2008.
- Leffler DA, Kelly CP, Green PHR, et al. Larazotide acetate for persistent symptoms of coeliac disease despite a gluten-free diet: a randomized controlled trial. Gastroenterology. 2015;148(7):1311–1319. PMID: 25683116.
- Innovate Biopharmaceuticals. Positive effect of larazotide acetate on reducing intestinal permeability in a NASH/NAFLD preclinical (DIAMOND mouse) study. EASL poster, 2019. (Cited as ref 8 in text.)
- Larazotide acetate protects the intestinal mucosal barrier from anoxia/reoxygenation injury via various cellular mechanisms. Biomedicines. 2025. PMC12561949. (Cited as ref 9 and 14 in text.)
- Antibacterial hyaluronic acid hydrogel with sustained release of larazotide as an effective colitis treatment. Int J Biol Macromol. 2025. ScienceDirect S016836592500817X.
- Karwowska M, Hardonniere K, et al. Viral spike antigen clearance and augmented recovery in children with post-COVID multisystem inflammatory syndrome treated with larazotide. Sci Transl Med. 2025;17(809):eadu4284. PMID: 40737433. DOI: 10.1126/scitranslmed.adu4284.
- The PAR2 antagonist larazotide can mitigate acute histamine-stimulated epithelial barrier disruption in keratinocytes: a potential adjunct treatment for atopic dermatitis. 2025. PMID: 40330848.
- Larazotide (AT-1001) is an eight-amino-acid peptide that antagonises the zonulin/PAR2 pathway to tighten intestinal tight junctions and lower gut permeability.
- It is the only molecule in the popular “leaky gut” conversation to reach a large phase III clinical trial — in coeliac disease, in patients re-exposed to gluten.
- That phase III programme was discontinued after an interim analysis showed it could not meet its primary endpoint; the failure moderates the hype without invalidating the underlying tight-junction biology.
- Newer preclinical and exploratory work spans MIS-C in children, NAFLD prevention in mice, colitis hydrogels and atopic-dermatitis barrier models, but is far earlier and more speculative.
- Larazotide is not an approved medicine for any indication; Condor supplies it as a research-use-only reference material with a Certificate of Analysis.
What is larazotide (AT-1001)?
Larazotide, also known as AT-1001, is an eight-amino-acid peptide studied as a tight-junction regulator. It is designed to antagonise the zonulin/PAR2 pathway and reduce intestinal permeability, making it the most clinically advanced candidate associated with “leaky gut” research. It is not an approved medicine and is supplied for research use only.
How is larazotide thought to work?
Larazotide is proposed to tighten the gut's tight junctions — the protein seals between intestinal cells — by opposing zonulin signalling and antagonising the PAR2 receptor, both of which can otherwise loosen the barrier. Barrier, keratinocyte and anoxia-reoxygenation studies support this mechanism, though mechanism alone does not establish clinical benefit.
Did larazotide work in coeliac disease?
Larazotide is the only leaky-gut peptide to reach a large phase III clinical trial, conducted in coeliac patients. That phase III programme was discontinued after an interim analysis concluded it could not meet its primary endpoint. The result moderates the hype around larazotide without invalidating the underlying tight-junction biology, and it remains the single most important fact in its file.
What other conditions is larazotide being researched for?
Beyond coeliac disease, larazotide has appeared in far earlier, more speculative research: a Science Translational Medicine study in children with post-COVID MIS-C, NAFLD/NASH prevention in a preclinical mouse model, colitis hydrogels, and atopic-dermatitis barrier models. These are mostly single studies, animal models or small exploratory cohorts and should not be read as established uses.
Is larazotide an approved drug, and how does Condor supply it?
No. Larazotide is not an approved medicine for any indication in the EU or elsewhere. Condor supplies it strictly as a research-use-only reference material — not for human or veterinary use — with a Certificate of Analysis documenting identity and purity, which is essential for any meaningful work with a peptide this short.