What Is GHRP-2 (Pralmorelin)? The Growth Hormone-Releasing Peptide, Examined
GHRP-2 (pralmorelin, KP-102) is a synthetic ghrelin-mimetic GH secretagogue. What the peptide is, how it works, and its Japan-only diagnostic status, examined.
GHRP-2, also called pralmorelin or KP-102, is a synthetic hexapeptide that mimics ghrelin at the growth hormone secretagogue receptor. In Japan it is an approved single-dose diagnostic agent for growth hormone deficiency. It has no therapeutic approval anywhere.
GHRP-2 is one of the most thoroughly characterized members of the growth-hormone-releasing peptide family, and unlike most compounds in that family it has an actual regulatory paper trail: a Japanese approval, a defined diagnostic protocol, and a developer who published the full chemistry. It is a synthetic hexapeptide that behaves like ghrelin at a specific pituitary receptor, and its story is really the story of how a laboratory tool for probing growth hormone reserve was built. Everything below describes laboratory and literature findings, not use in people.
What is GHRP-2, structurally?
GHRP-2 is a synthetic hexapeptide — six amino acids — and it goes by an unusually long list of names: pralmorelin (its international nonproprietary name), KP-102, GPA-748, and the developmental codes attached to it over the years. The base compound carries CAS number 158861-67-7; the diagnostic drug form is the dihydrochloride salt.1
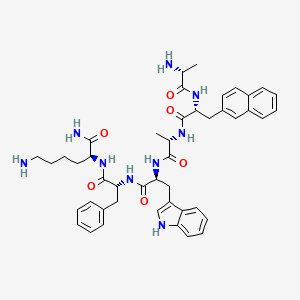
The sequence, taken from the developer’s own primary paper and corroborated by the Japanese regulatory dossier, is D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH2 — formally D-alanyl-3-(2-naphthyl)-D-alanyl-L-alanyl-L-tryptophyl-D-phenylalanyl-L-lysinamide.1,3 Two structural details matter and are frequently mangled in secondary sources. Position 2 is D-2-naphthylalanine, a bulky non-natural residue, not plain phenylalanine. And the C-terminus is amidated (the -NH2), not a free carboxylic acid. Both features are what you would expect from a peptide engineered for receptor affinity and resistance to peptidase degradation rather than one lifted from a natural protein. The IUPHAR/BPS Guide to Pharmacology classifies pralmorelin as a met-enkephalin analogue, which places it in the same design lineage as the earlier growth-hormone-releasing peptides that grew out of enkephalin chemistry.4
6 amino acids — GHRP-2 is a hexapeptide, but two of its residues are non-natural D-amino acids that no ribosome would ever assemble.
How does it work?
GHRP-2 is a ghrelin mimetic. It is an agonist at the growth hormone secretagogue receptor, GHS-R1a, expressed in the pituitary and hypothalamus. That receptor was cloned by Howard and colleagues in 1996 as “a receptor in pituitary and hypothalamus that functions in growth hormone release.”5 At the time its natural ligand was unknown; it was defined by the synthetic secretagogues, GHRP-2 among them, that activated it. Three years later Kojima and colleagues identified ghrelin, an acylated peptide from the stomach, as the endogenous ligand.6 GHRP-2 therefore does artificially what ghrelin does naturally: it binds GHS-R1a and drives growth hormone release.
The Japanese regulatory review makes the mechanistic attribution explicit, treating KP-102 as a ghrelin/GHS-R agonist and citing both the Howard and Kojima papers directly.3 A 2018 clinical study describing the GHRP-2 test states the same thing in operational terms — that GHRP-2 stimulates its targets through GHS-R in the hypothalamus, ghrelin’s natural ligand.12
In the developer’s own pharmacology, GHRP-2 in conscious rats was more potent than exogenous GHRH at releasing growth hormone, was relatively resistant to suppression by somatostatin, and produced no response in hypophysectomized rats — confirming the pituitary as its site of action.1,2 The relative somatostatin resistance is pharmacologically interesting: somatostatin is the brake on GH release, and a secretagogue that partly bypasses that brake produces a robust, reproducible GH pulse. That reproducibility is exactly what a diagnostic test needs.
GHRP-2 was defined by the receptor it activated years before anyone knew what that receptor was naturally for.
The regulatory reality: a Japan-only diagnostic
This is where GHRP-2 diverges sharply from the gray-market framing it usually receives. Pralmorelin hydrochloride is an approved drug — but in Japan only, and for one narrow purpose. Kaken Pharmaceutical markets it as “GHRP Kaken 100,” approved in 2004, with the indication “diagnosis of growth hormone secretion deficiency.”3,4 It is a single-dose diagnostic agent, administered once to provoke a measurable growth hormone response. It is not approved as a treatment for anything, and it is not approved in the European Union or the United States.
The diagnostic protocol in the PMDA label is specific: 100 µg given intravenously in the fasting state (2 µg/kg for ages 4 to under 18, capped at 100 µg), with growth hormone sampled at 0, 15, 30, 45 and 60 minutes. Severe GH deficiency is defined by a peak GH at or below 15 ng/mL, or at or below 9 ng/mL when measured against a recombinant GH standard.3
| Property | What the record shows |
|---|---|
| Names | GHRP-2, pralmorelin, KP-102, GPA-748 |
| Class | Synthetic hexapeptide GH secretagogue; ghrelin mimetic |
| Target | GHS-R1a (growth hormone secretagogue / ghrelin receptor) |
| Approved use | Japan only — single-dose diagnostic for GH deficiency |
| Approved elsewhere | No EU or US approval; no therapeutic approval anywhere |
Summary of the documented record for GHRP-2 / pralmorelin. The “approved use” line refers to a single-dose diagnostic test in Japan and must not be read as endorsement of any therapeutic or non-clinical use.
In human diagnostic studies GHRP-2 raises plasma growth hormone reliably and markedly, and does so largely independent of sex, age or obesity — the property that makes it a dependable provocative test where other stimuli can be blunted.7 An early study in 24 children of short stature found that intravenous and intranasal GHRP-2 evoked GH responses as reliable as GHRH for predicting pituitary reserve, with GHRH and GHRP-2 acting synergistically when combined.7 A modern validation in 36 patients with hypothalamic-pituitary disorder confirmed the test’s usefulness for diagnosing GH deficiency.11
Where GHRP-2 sits among the secretagogues
The GHRP series traces back to work begun by C.Y. Bowers at Tulane University in the late 1970s, and Bowers’s name recurs as a co-author across the core GHRP-2 clinical papers, reflecting his role in co-developing KP-102.7,8,9 Against its siblings, GHRP-2 is distinguished by potency and by its off-target profile. In a direct in-vitro comparison in rat primary pituitary cells, GHRP-2 was more potent than GHRP-6 at releasing growth hormone.13
The contrast with ipamorelin is instructive. Ipamorelin is a more selective secretagogue with minimal effect on ACTH and cortisol.14 GHRP-2 is not so clean: in humans it is a potent GH releaser that also modestly stimulates ACTH and cortisol, though not prolactin.10 That off-target activity on the hypothalamic-pituitary-adrenal axis was once a confounder; more recently it has been turned into a feature, with the ACTH response during the GHRP-2 test used to screen for secondary adrenal insufficiency at the same time.11,12 If you want to read GHRP-6, ipamorelin, and CJC-1295 against this same axis, see the GHRP-6 guide, the ipamorelin guide, and the CJC-1295 DAC guide, or the broader overview of growth hormone secretagogues.
An honest read of the evidence
The strong parts of the GHRP-2 record are the mechanism and the diagnostic use. The GHS-R1a target is well established, the ghrelin-mimetic identity is settled, and the Japanese approval as a single-dose diagnostic rests on a real regulatory dossier and reproducible GH-provocation data. That much is solid.
The weak parts are everything beyond acute diagnosis. There is no approved therapeutic indication for GHRP-2 anywhere, and there is no robust long-term human safety or efficacy data outside the acute diagnostic setting. Framing GHRP-2 as a “growth hormone therapy” or a performance agent is unsupported by any regulator; the primary evidence supports only acute GH provocation. Several of the foundational clinical papers date from the 1990s and are small — 24 children in one, similar numbers in others — and frequently list the compound’s own discoverer, Bowers, as a co-author.7,8,9 Large independent modern efficacy trials outside the diagnostic indication are lacking, and development for short stature was discontinued.
There is also a sourcing concentration worth naming. Much of the detailed potency and general-pharmacology data comes from the developer, Kaken, published in a single 2004 journal, and from animal models — rats and dogs.1,2 Single-sponsor sourcing plus species differences are real limitations on how far those numbers generalize. And GHRP-2 is not receptor-selective for growth hormone: it also raises ACTH, cortisol and in some settings prolactin, so any GH signal has to be interpreted against that off-target activity rather than treated as a clean GH-only readout.10 Finally, gray-market “GHRP-2” is not the diagnostic drug product. Identity, purity and endotoxin status of research-grade material are unverified in the absence of a compound-specific certificate of analysis, and no such claim is made here.
All materials supplied by Condor Research are Research Use Only (RUO). Everything above describes in-vitro findings, animal studies, and the published regulatory and clinical literature — it is not a dosing protocol, clinical guidance, or a safety assessment for any organism. Nothing here concerns human or veterinary use.
Condor Research · Scientific desk
Atrio Sciences s.r.o., IČO 57 669 651, Nitra (SK) · info@condorresearch.com
- GHRP-2 = pralmorelin = KP-102 = GPA-748; a synthetic hexapeptide growth hormone secretagogue, CAS 158861-67-7 (base).
- Verified sequence: D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH2, C-terminally amidated, chemically a met-enkephalin analogue.
- It acts as a ghrelin-mimetic agonist at the growth hormone secretagogue receptor GHS-R1a in pituitary and hypothalamus.
- In Japan only, pralmorelin hydrochloride is an approved single-dose diagnostic drug for growth hormone deficiency — not a therapeutic, and not approved in the EU or US.
- It is more potent than GHRP-6 at releasing GH from rat pituitary cells, and unlike ipamorelin it also modestly raises ACTH and cortisol.
- In humans it reliably raises plasma GH regardless of sex, age or obesity, which is why it works as a provocative diagnostic test.
Is GHRP-2 the same thing as pralmorelin?
Yes. Pralmorelin is the international nonproprietary name for GHRP-2, which is also coded KP-102, GPA-748 and WAY-GPA-748. The base compound is CAS 158861-67-7; the diagnostic drug is the dihydrochloride salt.
What is GHRP-2's amino acid sequence?
D-Ala-D-2-Nal-Ala-Trp-D-Phe-Lys-NH2, a C-terminally amidated hexapeptide containing two non-natural D-amino acid residues, including D-2-naphthylalanine at position two. It is chemically classified as a met-enkephalin analogue.
How does GHRP-2 cause growth hormone release?
It acts as an agonist at the growth hormone secretagogue receptor GHS-R1a in the pituitary and hypothalamus, the same receptor activated by the natural hormone ghrelin. Studies in rats show it is more potent than exogenous GHRH and relatively resistant to somatostatin suppression.
Is GHRP-2 an approved medicine?
Only in Japan, where pralmorelin hydrochloride ("GHRP Kaken 100") was approved in 2004 as a single-dose diagnostic agent for growth hormone deficiency. It is not approved as a therapeutic, and it is not approved in the European Union or the United States.
How is GHRP-2 different from GHRP-6 and ipamorelin?
In rat pituitary cells GHRP-2 releases growth hormone more potently than GHRP-6. Compared with ipamorelin, which is highly selective, GHRP-2 is less clean — it also modestly stimulates ACTH and cortisol, an off-target effect on the adrenal axis that ipamorelin largely lacks.
Why does GHRP-2 also affect cortisol?
Because it is not receptor-selective for growth hormone. In human studies GHRP-2 modestly activates the hypothalamic-pituitary-adrenal axis, raising ACTH and cortisol. In modern diagnostic use this is sometimes exploited to screen for secondary adrenal insufficiency during the same test.