PT-141 (Bremelanotide): The Melanocortin That Targets Desire, Not Plumbing
An FDA-approved cyclic peptide that acts in the brain rather than the blood vessels: a narrow indication, a modest effect, and a melanocortin tax of nausea and pigment.
PT-141 (bremelanotide) is a synthetic cyclic melanocortin-receptor agonist, approved in the US as Vyleesi for hypoactive sexual desire disorder in premenopausal women. Unlike PDE5 inhibitors, it acts centrally on brain melanocortin pathways rather than on vasculature. The licensed effect is modest, and nausea, transient blood-pressure rise, and focal hyperpigmentation are documented. The research-grade reference material is not the medicine.
Most molecules that touch human sexual response work on the plumbing. Sildenafil and its PDE5 relatives relax vascular smooth muscle and let blood do the rest: peripheral, mechanical, downstream. Bremelanotide does something stranger. It reaches up into the brain’s melanocortin circuitry and tugs on desire itself, before any vessel has dilated. That is the whole pitch, and also the whole problem.
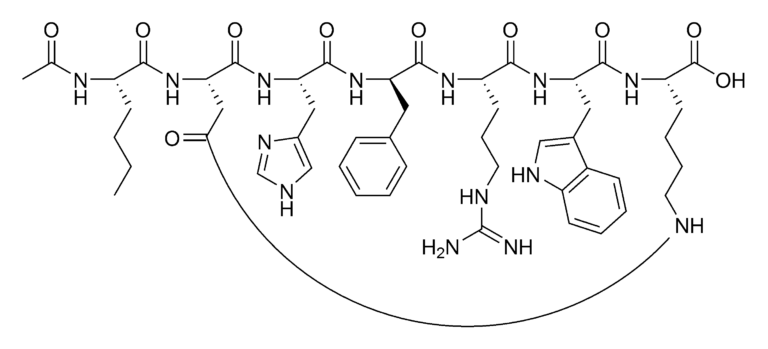
PT-141, better known by its INN bremelanotide and its US brand name Vyleesi78, is a synthetic cyclic heptapeptide and a non-selective melanocortin-receptor agonist.711 It descends from the same melanocortin scaffold as Melanotan II311, and like its better-known relative it engages MC4R and MC1R and carries the family’s characteristic baggage.411 Where the tanning peptide was chased for pigmentation, PT-141 was developed for a quite different endpoint: it is approved in the United States for hypoactive sexual desire disorder (HSDD) in premenopausal women.67 Approved is the operative word here, and, as we will see, also the most easily misread one.
Why does a central mechanism change the whole conversation?
The clearest way to understand PT-141 is by contrast with what it is not. A PDE5 inhibitor never asks whether you want anything; it simply removes a vascular brake, operating on smooth muscle in the periphery. Bremelanotide inverts that logic. By acting as an agonist at central melanocortin receptors, principally MC4R3, which is expressed densely in hypothalamic regions such as the paraventricular nucleus311, it is theorised to modulate the upstream circuitry of motivation and arousal rather than the downstream hardware.313
This is why the two drug classes are not competitors so much as different categories of intervention. One addresses a question of capacity; the other a question of drive. That distinction is also why bremelanotide’s side-effect signature looks nothing like a PDE5 inhibitor’s. A molecule that engages central melanocortin receptors and MC1R does not get to touch desire without also touching pigmentation, nausea pathways, and cardiovascular tone. The mechanism is the marketing and the mechanism is the liability, in equal measure.
PT-141 is the rare sexual-function molecule that targets wanting rather than working, and it pays for that ambition in nausea and pigment.
What did the RECONNECT trials actually show?
The pivotal evidence for the approved indication came from a pair of identical phase 3 trials run under the RECONNECT programme in premenopausal women with HSDD67, enrolling 1,267 women in total.17 The honest summary is that they were positive on their co-primary endpoints, which were change in a validated desire score (the Female Sexual Function Index desire domain14) and change in desire-related distress (an item from the Female Sexual Distress Scale12), and that the magnitude of those improvements was modest. These were statistically significant, patient-reported shifts, not transformative ones.15
Crucially, the regulatory record is precise about what bremelanotide did not do. The number of satisfying sexual events, the more concrete behavioural metric, was a secondary endpoint1, and it showed no significant difference between bremelanotide and placebo.15 This is the part of the story that hype tends to launder. Regulatory approval certifies that a benefit is real and outweighs harm for a defined population under defined conditions; it does not certify that the benefit is large. For PT-141, the gap between “works” and “works a lot” is exactly where an honest appraisal lives.
| Property | PT-141 (bremelanotide) | PDE5 inhibitors |
|---|---|---|
| Site of action | Central (brain melanocortin pathways) | Peripheral (vascular smooth muscle) |
| Molecular target | Melanocortin receptors (MC4R/MC1R) | Phosphodiesterase type 5 |
| Endpoint affected | Desire / motivation | Physiological capacity |
| Approved indication | HSDD in premenopausal women (US) | Erectile dysfunction / others |
| Signature liability | Nausea, BP rise, hyperpigmentation | Headache, flushing, visual effects |
Mechanism comparison: two routes to broadly the same clinical territory, with entirely different biology and risk profiles.
How bad is the adverse-event profile, plainly stated?
Three liabilities are documented and worth stating without softening. First, nausea: about 40% of participants experienced it, most commonly after the first dose64, making it the most frequent treatment-related adverse event and the leading reason participants discontinued.62 A drug whose leading adverse event is also its leading cause of dropout has a tolerability problem, not a footnote. Second, a transient rise in blood pressure with a corresponding fall in heart rate in the hours after exposure, a melanocortin-mediated cardiovascular effect that constrains who can be studied safely.68 Third, focal hyperpigmentation: because MC1R is the receptor that drives melanogenesis, engaging it can darken skin and gums42, the most direct fingerprint of the molecule’s shared lineage with the melanocortin family.1114
~40% of subjects reported nausea, most commonly after the first dose: the most frequent adverse event and the leading reason for discontinuation.
None of these are exotic surprises. They are the predictable cost of a non-selective melanocortin agonist that reaches the central nervous system.43 The pigmentation in particular is a useful honesty test: a molecule cannot be sold as “just for desire” when its receptor promiscuity is written on the patient’s skin.
What does an honest appraisal leave on the table?
Several things, and they matter. The approved population is narrow, premenopausal women with acquired, generalised HSDD28, so the evidence does not transfer cleanly to other groups, and extrapolation beyond that population is speculation rather than data.125 The effect sizes were modest and leaned heavily on subjective, patient-reported instruments rather than hard behavioural endpoints, the most concrete of which was not significantly improved. The cardiovascular signal excludes people with uncontrolled hypertension or known cardiovascular disease from the licensed use68, which tells you the safety margin is real and bounded. And the longer-term picture, durability of effect and the cumulative pigmentation question, remains thinner than anyone selling certainty would admit.
The fair verdict is therefore neither dismissal nor enthusiasm. PT-141 is a legitimately approved drug with a genuine, mechanistically novel effect, a modest benefit, and a tolerability tax that a meaningful fraction of subjects declined to pay.15 That is a more interesting and more defensible story than the one usually told about it.
So what does this mean for research handling?
Everything above concerns the licensed medicine and the named clinical trials that produced it: populations studied under controlled conditions, not outcomes a reader should expect or pursue. A research-grade bremelanotide reference is a different object entirely. It exists to support analytical and laboratory work, supplied strictly as Research Use Only, with no human application, no dosing, and no therapeutic claim attached. The approved drug and the reference material share a structure and a name; they do not share a purpose.
What makes a reference batch usable is documentation, not branding. For a cyclic peptide of this kind, identity and purity are the entire question: a current Certificate of Analysis, HPLC purity data, and mass-spectrometric confirmation of identity109 are what allow one laboratory’s result to be reproduced in another. Without that paper trail, a sample is an unknown wearing a known name. With it, the molecule becomes something a researcher can reason about, which is the only honest reason to handle it at all.
- PT-141/bremelanotide is a synthetic cyclic heptapeptide and non-selective melanocortin-receptor agonist (MC4R/MC1R) that shares the melanocortin lineage of Melanotan II.
- Its mechanism is central: it engages brain melanocortin circuitry, which categorically distinguishes it from PDE5 inhibitors that act peripherally on vascular smooth muscle.
- It is genuinely FDA-approved (Vyleesi) but only for HSDD in premenopausal women, a narrow indication with modest, patient-reported effect sizes in the RECONNECT trials.
- Honesty caveat: the co-primary endpoints were desire and distress; the number of satisfying sexual events, a secondary endpoint, was not significantly improved.
- The adverse-event profile is real: nausea in about 40% of subjects (most common after the first dose and the leading reason for discontinuation), transient blood-pressure rise with a fall in heart rate, and focal hyperpigmentation from MC1R engagement.
- The approved medicine and a research-grade analytical reference are not interchangeable; identity and purity documentation (COA, HPLC/MS) is what makes a reference batch usable for reproducible work.
Is research-grade PT-141 the same thing as the approved drug Vyleesi?
No. Vyleesi (bremelanotide) is a licensed medicine, formulated, dosed, and regulated for a specific clinical indication. A research-grade PT-141 reference shares the same peptide structure and name but is supplied strictly as Research Use Only material for laboratory and analytical work, with no human application, no dosing information, and no therapeutic claim. Same molecule, fundamentally different purpose and regulatory status.
How does PT-141's mechanism differ from Viagra-type drugs?
They occupy different biological categories. PDE5 inhibitors such as sildenafil act peripherally on vascular smooth muscle, addressing physiological capacity. Bremelanotide acts centrally as a melanocortin-receptor agonist, engaging brain pathways associated with desire and motivation rather than blood flow. One removes a vascular brake downstream; the other is theorised to modulate the upstream circuitry of drive itself. This is why their side-effect profiles diverge so sharply.
What did the strongest human trials actually demonstrate?
The pivotal RECONNECT phase 3 trials, in premenopausal women with HSDD, met their co-primary endpoints of improved desire scores and reduced associated distress. Honestly stated, the improvements were statistically real but modest and rested on subjective patient-reported instruments. The number of satisfying sexual events, a secondary endpoint, was not significantly improved. Approval confirms a benefit exists for that narrow population; it does not imply the benefit is large.
What adverse effects were documented in the studies?
Three are well established and trace to the molecule's melanocortin lineage. Nausea was the most common, affecting about 40% of subjects (most often after the first dose) and the leading cause of discontinuation. A transient rise in blood pressure with a fall in heart rate was observed in the hours after exposure. Focal hyperpigmentation of skin and gums can occur via MC1R engagement, the same receptor activity shared across the melanocortin family.