
Two Hormones, One Vial: The Tirzepatide Evidence, Read Honestly
Tirzepatide beat semaglutide head-to-head on weight loss in a randomised trial. Here is what the human data actually establish — and the hard line between a licensed medicine and a research-grade reference compound.
Tirzepatide is a dual GIP/GLP-1 receptor agonist licensed as a medicine (Mounjaro, Zepbound) and supported by large randomised trials. In SURMOUNT-5 it produced greater weight loss than semaglutide (20.2% versus 13.7% at 72 weeks). A research-grade vial is an analytical reference material, not that medicine: no approved use, no patient outcomes, and weight regain after stopping is documented.
For two decades the incretin field chased a single hormone, GLP-1, and was rewarded with real but bounded results. Then a molecule that deliberately hits two receptors at once — GIP and GLP-1 — walked into a head-to-head trial against the best single-agonist on the market and won on the one endpoint everyone was watching: 20.2% mean weight loss versus 13.7%.102 That result, more than any mechanistic diagram, is why tirzepatide reset expectations for what an incretin drug could do.4
What does the human evidence actually show?
Tirzepatide is unusually well-characterised for a compound that gets discussed in research-vial circles. It is an approved medicine — marketed as Mounjaro for type 2 diabetes and Zepbound for chronic weight management41 — backed by two large randomised programmes. The SURPASS programme tested it in diabetes, where it outperformed semaglutide on both glycaemic control and weight in SURPASS-2.111 The SURMOUNT programme tested it in obesity without diabetes. In SURMOUNT-1, the pivotal obesity trial, participants on the highest dose (15 mg) reached a mean weight reduction of up to 22.5% over 72 weeks.24 This is not a preclinical signal or a mechanistic promise; it is a placebo-controlled outcome in thousands of randomised humans.4
For context, semaglutide reached roughly 15-17% in its own STEP obesity trials23, so tirzepatide’s top-dose figure sits visibly higher — though that is a cross-trial comparison between separate placebo-controlled studies, not a head-to-head result. The decisive datum is the one that closed that gap directly. SURMOUNT-5 randomised participants against semaglutide itself — not placebo, but the incumbent — and tirzepatide produced 20.2% mean weight loss versus 13.7% at 72 weeks.102 Beating placebo is table stakes; beating the reigning standard of care on the same protocol is what moved the field.
22.5% mean body-weight reduction at the 15 mg top dose in the SURMOUNT-1 obesity trial over 72 weeks.2
Why does adding GIP to GLP-1 matter?
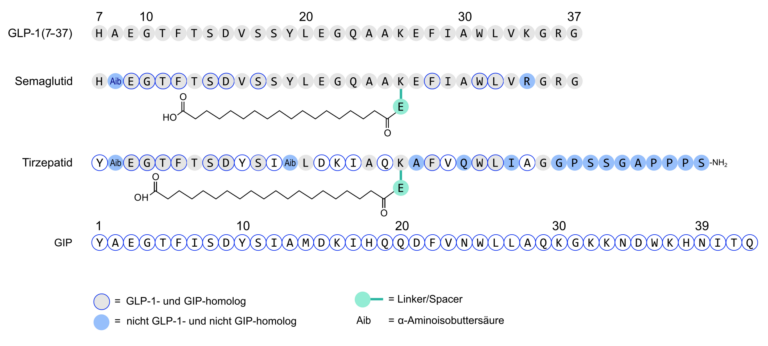
The conceptual leap is that tirzepatide engages two distinct incretin receptors rather than one. GLP-1 receptor agonism — the mechanism behind semaglutide — slows gastric emptying, enhances glucose-dependent insulin secretion and acts centrally to reduce appetite.4 Tirzepatide preserves that and layers on glucose-dependent insulinotropic polypeptide (GIP) receptor activity, a second incretin axis with its own effects on insulin secretion and adipose-tissue metabolism.45 The working hypothesis is that the two signals are at least additive, and possibly synergistic, on glycaemic control and energy balance.4
It is worth being precise about confidence here. The clinical superiority is established; the mechanistic attribution is not fully resolved.4 GIP biology is genuinely counter-intuitive — both agonism and antagonism of the GIP receptor have been argued to aid metabolic outcomes4 — and tirzepatide itself behaves as an imbalanced, biased agonist rather than a clean dual activator4, which complicates any tidy account. Disentangling how much of its edge comes from the GIP arm versus a more favourable GLP-1 pharmacology is still an active question. The trial result is firm; the “two is better than one” story is the leading interpretation, not a closed case.
| Agent | Receptor target | Anchor evidence |
|---|---|---|
| Semaglutide | GLP-1 (single) | STEP / SUSTAIN programmes; ~15-17% in STEP obesity trials |
| Tirzepatide | GIP + GLP-1 (dual) | SURMOUNT / SURPASS; 20.2% vs 13.7% over semaglutide in SURMOUNT-5103 |
| Retatrutide | GIP + GLP-1 + glucagon (triple) | Phase 2 obesity data (up to ~24.2%); not yet approved4 |
Incretin agonism by receptor count and the trials anchoring each — single, dual and the emerging triple agonist.
Tirzepatide’s importance is not that it added a receptor, but that the addition translated into a randomised win over the best single-agonist available.
What is the documented adverse-event and durability profile?
The tolerability signature is dominated by the gastrointestinal tract. Across the SURMOUNT and SURPASS trials, nausea, vomiting, diarrhoea and constipation were the most frequently reported adverse events67, typically most pronounced during dose escalation and generally mild-to-moderate, though they accounted for most treatment discontinuations.6 This is broadly the class profile of incretin agonists rather than something unique to dual agonism.
The harder question is durability. SURMOUNT-4 examined withdrawal directly: after an initial lead-in, participants who continued tirzepatide held and extended their weight loss, while those switched to placebo regained a mean of around 14 percentage points of body weight over the following year.24 That reframes these compounds as chronic interventions in the populations studied rather than one-off corrections48, and the rebound is one of the most consequential open findings of the whole class.6
How honest is the evidence — and what is missing?
Four caveats deserve to be stated plainly. First, almost all of the headline data come from a single sponsor’s trial programme6; independent replication and longer real-world follow-up are still maturing.614 Second, the mechanistic question above is unresolved — the field has a superior molecule without a settled account of why the GIP component helps. Third, the pivotal SURMOUNT and SURPASS trials measured weight and glycaemia, not hard cardiovascular endpoints915; long-term cardiovascular and mortality outcomes are only now arriving, with SURPASS-CVOT reporting and SURMOUNT-MMO still ongoing.159 Fourth, durability beyond a year or two, and the full safety ledger at population scale, accumulate more slowly than the marketing cycle.
Looking forward, the obvious trajectory is more receptors, not fewer. Retatrutide adds glucagon-receptor agonism to the GIP/GLP-1 pairing4, and its phase 2 obesity data reached mean reductions of up to about 24.2% at 48 weeks4 — figures that, if they survive larger trials, would exceed tirzepatide’s. But retatrutide is not approved, its evidence base is far thinner, and extrapolating from a single phase 2 trial is exactly the kind of over-reach this field should have learned to resist. The multi-agonist story is compelling precisely because each step so far has been earned in a randomised trial — a standard worth holding the next molecules to.
A closing distinction matters more than any effect size. Everything above describes the licensed medicine studied in named trials in defined patient populations; it is not a use protocol, and nothing here describes outcomes a reader should expect. A research-grade tirzepatide vial is an analytical reference material — handled for laboratory characterisation, not administration — and it carries no approved indication of its own. For that work the only thing that counts is what the molecule actually is: identity and purity established by a current Certificate of Analysis with HPLC and mass-spectrometry data6, so that results are traceable, reproducible and not confounded by an unverified input.
- In SURMOUNT-5, tirzepatide produced greater weight reduction than semaglutide head-to-head (20.2% versus 13.7% at 72 weeks) — the strongest evidence that dual agonism beats GLP-1 alone.
- Top-dose tirzepatide reached up to 22.5% mean weight reduction in the SURMOUNT-1 obesity trial, a larger figure than the ~15-17% seen with single-incretin agents in their own placebo-controlled trials (a cross-trial, not head-to-head, comparison).
- The mechanistic hypothesis — that adding GIP to GLP-1 agonism is additive or synergistic — is plausible and trial-consistent, but the precise contribution of the GIP arm in humans remains debated.
- Gastrointestinal adverse events (nausea, vomiting, diarrhoea) dominate the documented tolerability profile and drive most discontinuations in trials.
- Honest caveat: weight regain after discontinuation is documented in SURMOUNT-4, and long-term cardiovascular and mortality outcomes are still maturing in ongoing trials.
- The licensed drug is not the research vial: a reference compound has no approved indication, and its value depends entirely on identity and purity documentation (COA, HPLC/MS).
Is a research-grade tirzepatide vial the same thing as Mounjaro or Zepbound?
No. Mounjaro and Zepbound are licensed, quality-controlled finished medicines approved by regulators and supported by the SURPASS and SURMOUNT trials. A research-grade vial is an analytical reference material with no approved indication, no marketing authorisation and no clinical use. The trial evidence describes the medicine in defined patient populations, not the reference compound, which is intended for laboratory characterisation only.
What is the single strongest piece of human evidence for tirzepatide?
The SURMOUNT-5 trial, which randomised participants to tirzepatide versus semaglutide directly rather than against placebo. Tirzepatide produced 20.2% mean weight loss versus 13.7% at 72 weeks. Beating the incumbent standard of care, not merely placebo, is what makes this the field's most decisive datum and the clearest evidence that dual GIP/GLP-1 agonism can outperform GLP-1 alone in the populations studied.
What adverse effects were most commonly documented in the trials?
Gastrointestinal events dominated: nausea, vomiting, diarrhoea and constipation were the most frequent, generally mild-to-moderate and most pronounced during dose escalation, though they drove most discontinuations. This mirrors the broader incretin class rather than being unique to dual agonism. These are observations from named clinical trials in their study populations, not predictions of what any individual would experience.
Does the weight loss persist after the compound is stopped?
SURMOUNT-4 examined this specifically: participants switched from tirzepatide to placebo regained a mean of roughly 14 percentage points of body weight over the following year, while those who continued held and extended their loss. This is direct tirzepatide withdrawal evidence, consistent with the wider incretin class, and reframes these agents as chronic interventions in the populations studied rather than durable one-off corrections.