What Is Cardiogen? The AEDR Heart Peptide, Examined Honestly
Cardiogen is the AEDR tetrapeptide from the Khavinson family. Real chemistry, but its cardiac evidence is thin, single-lab, and unreplicated. An honest look.
Cardiogen is a synthetic tetrapeptide, Ala-Glu-Asp-Arg (AEDR), from the Khavinson bioregulator family. Its chemistry is verifiable, but its cardiac evidence rests on a handful of single-lab tissue-culture studies, with no human trials, no independent replication, and no live-heart disease model.
Cardiogen is one of the more confidently marketed members of the Khavinson short-peptide family: a four-residue „heart peptide” pitched as a way to distil the activity of a whole calf-heart extract into a single defined molecule. The chemistry underneath that pitch is real and checkable. The cardiac efficacy underneath it is not — the trail is thin, it runs through one laboratory, and the few studies that exist mostly use the wrong model or the wrong endpoint. Everything below describes laboratory and literature findings, not use in people or animals.
What is Cardiogen, structurally?
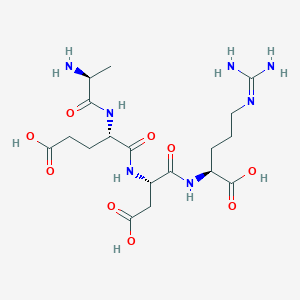
Cardiogen is a synthetic tetrapeptide with the sequence Ala-Glu-Asp-Arg — AEDR in one-letter code, written formally as H-Ala-Glu-Asp-Arg-OH. Its molecular formula is C18H31N7O9 and its molecular weight is roughly 489.5 Da; it is catalogued in PubChem as compound CID 11583989.1 No CAS number is assigned to it, and you should be wary of any vendor listing that invents one.
The sequence itself is not fictional. The AEDR tetrapeptide has been studied directly as a short DNA-binding peptide, appearing in work on how such peptides interact with histones and oligonucleotides in vitro.2 So the first layer of the Cardiogen story — that there is a specific, defined molecule behind the trade name — holds up. That is worth stating clearly, because it is the part of the claim that is actually true.
Cardiogen sits inside the family of „ultrashort” bioregulators developed at the St. Petersburg Institute of Bioregulation and Gerontology, associated with Vladimir Khavinson. It shares its acidic Ala-Glu-Asp core with siblings such as Epithalon (AEDG, framed as pineal) and Bronchogen (AEDL, framed as bronchial). The differing C-terminal residue — arginine, in Cardiogen’s case — is the proposed handle for tissue specificity, the idea being that swapping one residue redirects an otherwise similar peptide toward a different organ.3 That is a hypothesis about specificity, not a demonstrated fact for AEDR and the heart.
489.5 the molecular weight in daltons of the AEDR tetrapeptide — the one part of the Cardiogen claim that is fully verifiable.
Cardiogen versus Chelohart: peptide versus extract
Cardiogen is best understood as the synthetic analogue of Chelohart, the crude calf-heart polypeptide extract from the same tradition. The central premise of the whole family is reductionist: that the activity of a messy, multi-component tissue extract can be captured in one short, defined peptide. Chelohart, the extract, has itself been examined in organotypic heart culture, where it was reported to raise a proliferation marker (PCNA) and lower p53 in cultured cardiac tissue from rats of different ages.4 Cardiogen is the attempt to reproduce that with a single molecule — but the two are not interchangeable, and evidence for one is not evidence for the other.
What does the primary literature actually show?
Here the marketing and the evidence part ways. The genuinely cardiac primary data for Cardiogen amount to very little. The clearest single study is an organotypic myocardial tissue-culture experiment: synthetic Cardiogen at a very low concentration (on the order of 10-12 M) was reported to stimulate cell proliferation and reduce p53 in heart tissue culture from young and old rats.5 A second paper places Cardiogen among a set of tissue-specific bioregulators tested in organotypic cultures of several organs, claiming tissue-directed stimulation of reparative processes.6 Both are ex-vivo cell culture — not a beating heart, not a disease model, and not a living animal.
The only in-vivo study naming Cardiogen that turns up is not about the heart at all. It examined the peptide’s effect on transplanted M-1 sarcoma in aged rats, reporting a tumor-modifying, anti-angiogenic action.7 That the trade name appears in an animal study is worth noting; that the endpoint is cancer, not cardioprotection, is worth noting more. Cardiogen also surfaces as a comparator peptide in work on human prostate fibroblast cultures — again, not heart tissue — which shows how loosely the name travels across tissues in this corpus.8
| Study type | Model | Endpoint | What it does and doesn’t show |
|---|---|---|---|
| Organotypic culture5 | Rat myocardial tissue, ex vivo | Proliferation up, p53 down | Cardiac tissue, but no live heart, no disease |
| Multi-tissue culture6 | Rat heart/lung/prostate/pancreas, ex vivo | Reparative stimulation | Places Cardiogen in the „tissue-specific” set; still culture only |
| In-vivo rat7 | M-1 sarcoma, transplanted | Tumor suppression | Living animal, but a cancer endpoint — not cardiac |
| In-silico docking3 | Computational transporter model | Predicted cellular transport | Lists AEDR among 26 peptides; no functional data |
All functional entries above are in-vitro, ex-vivo, computational, or non-cardiac. None is a live-heart disease model, and none is a human study. Research Use Only.
The proposed mechanism — and what is actually demonstrated
The mechanistic story offered for the Khavinson peptides is genuinely interesting and genuinely distinct from ordinary signalling peptides. Rather than binding a surface receptor, these short peptides are proposed to enter the nucleus and bind DNA or chromatin in a sequence-specific way, nudging gene expression — an epigenetic mode of action.9 There is real experimental support for this at the class level: fluorescently labelled short peptides such as Epithalon (AEDG), Pinealon (EDR) and Testagen (KEDG) were shown to penetrate the nucleus of HeLa cells and bind deoxyribo-oligonucleotides and DNA in vitro.10
AEDR was not among the peptides tested for nuclear entry — so Cardiogen’s mechanism is inherited by analogy, not shown for the molecule itself.
That distinction matters. The nuclear-penetration and DNA-binding experiments establish a plausible mechanism for the family, but Cardiogen’s specific sequence was not among those directly tested in that work. A separate in-vitro study did examine AEDR alongside other short peptides binding wheat histones and DNA complexes2 — but that is a plant-histone assay, nothing cardiac. The originating group’s own systematic review is the clearest place where the AEDR sequence is explicitly tied to the Cardiogen name and to „cardiovascular system function,”11 and there is a companion review sketching a rationale for peptides against cardiovascular cell senescence.12 Both are framing documents from the same lab, not independent primary evidence.
An honest read of the evidence
Strip away the presentation and a few structural weaknesses stand out. The first is a single-lineage problem: essentially all of the functional data trace back to Khavinson and immediate collaborators at one institute. There is no independent, Western, or replicated cardiac study of AEDR. When an entire evidence base originates from one group, the ordinary safeguards of science — replication by strangers with no stake in the result — simply have not run.
The second is a model-and-endpoint mismatch. The only cardiac-tissue data are ex-vivo organotypic cultures — not a living heart, not an infarct or heart-failure model. The only in-vivo Cardiogen study measured tumor suppression in sarcoma, which tells you nothing about cardiovascular function. So the „heart peptide” has never, in the published record, been tested against heart disease in a living animal.
The third is that the mechanism is inferred rather than shown for AEDR. Nuclear penetration and DNA binding are demonstrated for related peptides, and the cardiac gene-expression narrative is built by analogy from them. The fourth is venue and rigour: much of the corpus sits in low-visibility, largely Russian-language journals, at extremely low concentrations (10-12 M), with limited methodological detail and no external dose-response replication. And the fifth is the simplest: there is no safety, pharmacokinetic, toxicology, or human data of any kind. The „cardioprotective” framing common on vendor pages is not supported by a single primary human or in-vivo cardiac study.
There is also a trap worth naming for anyone researching this compound. A naive PubMed search for „Cardiogen heart” or „Cardiogen clinical” pulls up transthyretin cardiac amyloidosis and calmodulinopathy papers from the unrelated „cardiogenetics” field. Those papers are not about this peptide, share only incidental keywords, and must never be cited as evidence for AEDR. The confirmed reality is that a search for Cardiogen clinical efficacy returns the wrong literature entirely.
All materials supplied by Condor Research are Research Use Only (RUO). Everything above summarises in-vitro, ex-vivo, computational, and literature findings; none of it is a dosing protocol, clinical guidance, therapeutic claim, or safety assessment for any organism. Cardiogen is an unapproved investigational compound and is not intended for human or veterinary use. For the broader family context, see our overviews of Khavinson peptide bioregulators and which bioregulator maps to which tissue claim, and the same honest treatment applied to a sibling in what is Cortagen.
Condor Research · Dział naukowy
Atrio Sciences s.r.o., IČO 57 669 651, Nitra (SK) · info@condorresearch.com
- Cardiogen is a synthetic tetrapeptide with sequence Ala-Glu-Asp-Arg (AEDR), molecular formula C18H31N7O9, MW ~489.5 Da, PubChem CID 11583989; no CAS number is assigned.
- It belongs to the Khavinson short-peptide bioregulator family and shares the acidic Ala-Glu-Asp core with Epithalon (AEDG) and Bronchogen (AEDL); the C-terminal Arg is proposed to steer it toward cardiac tissue.
- The genuine cardiac primary evidence is essentially one ex-vivo organotypic myocardial culture study plus one multi-tissue culture study, both from the same Russian group.
- The only in-vivo cardiogen study measured tumor suppression in sarcoma, not any cardiovascular outcome.
- The proposed DNA-binding, epigenetic mechanism is demonstrated for sibling peptides, not for AEDR itself — the cardiac story is by analogy.
- There are zero human clinical trials; ClinicalTrials.gov returns no cardiogen-peptide study and the compound is not approved anywhere.
- A naive PubMed search for 'cardiogen + heart' surfaces unrelated transthyretin cardiac amyloidosis and 'cardiogenetics' papers that are not about this peptide.
Is Cardiogen the same as Chelohart?
No. Cardiogen is the synthetic tetrapeptide AEDR; Chelohart is the crude calf-heart polypeptide extract it was modelled on. Chelohart, the extract, has its own organotypic-culture literature, but evidence for the extract is not evidence for the single peptide, and vice versa.
Does Cardiogen have proven cardioprotective effects?
No. There is no primary in-vivo cardiac study or human study of AEDR demonstrating cardioprotection. The cardiac data are limited to ex-vivo tissue cultures from one research group, and the only in-vivo Cardiogen study had a cancer endpoint.
What is Cardiogen's amino acid sequence and formula?
The sequence is Ala-Glu-Asp-Arg (AEDR), written H-Ala-Glu-Asp-Arg-OH. The molecular formula is C18H31N7O9 and the molecular weight about 489.5 Da; it is listed in PubChem as CID 11583989. No CAS number is assigned.
Are there human clinical trials of Cardiogen?
None. ClinicalTrials.gov has no cardiogen-peptide entry, and PubMed queries combining cardiogen with clinical or human terms return only unrelated amyloidosis and calmodulinopathy literature. There is also no pharmacokinetic, toxicology, or safety dataset for the compound.
What is the proposed mechanism, and is it established?
The proposed mechanism is epigenetic: nuclear entry and sequence-specific DNA binding to modulate gene expression. This is experimentally supported for sibling peptides such as Epithalon and Pinealon, but AEDR itself was not among the peptides tested for nuclear penetration, so the mechanism is inferred by analogy rather than shown directly.
Why do search results show cardiac amyloidosis and "cardiogenetics" papers?
Because those come from a separate, unrelated field. Transthyretin cardiac amyloidosis and calmodulinopathy papers share incidental keywords with searches for the peptide but have nothing to do with the AEDR molecule. They should never be cited as evidence for Cardiogen's activity.