What Is Hexarelin? The GH Secretagogue With a Cardiac Side-Story
Hexarelin is a synthetic GHRP-family hexapeptide that releases GH via GHS-R1a — and, in rodent hearts, binds CD36. A cited, RUO-only research overview.
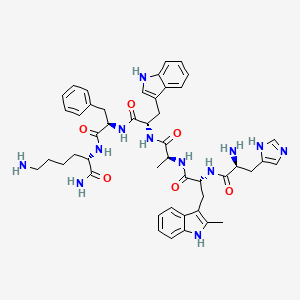
Hexarelin is a synthetic hexapeptide growth-hormone secretagogue of the GHRP family (sequence His-D-2-Me-Trp-Ala-Trp-D-Phe-Lys-amide). It releases GH via the GHS-R1a ghrelin receptor and, separately, binds the cardiac scavenger receptor CD36 in rodent studies. All findings here are laboratory or literature only.
Hexarelin sits at an unusual intersection in peptide pharmacology: it is a growth-hormone secretagogue that also, in rodent hearts, binds a receptor that has nothing to do with growth hormone. The first arm is well established — a six-residue peptide that triggers GH release through the ghrelin receptor. The second is stranger and more contested: a body of rat and mouse work pointing at CD36, a scavenger receptor, as the peptide’s cardiac binding partner. Both stories are real, but they are not equally mature. Everything below describes laboratory and literature findings, not use in people or animals.
What is hexarelin, structurally?
Hexarelin is a synthetic hexapeptide — six amino acids — with the sequence His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys and a C-terminal amide.1 The PubChem record (CID 6918297) lists the INN name examorelin, CAS number 140703-51-1, molecular formula C47H58N12O6, and a molecular weight near 887 g/mol; its IUPAC name, L-histidyl-2-methyl-D-tryptophyl-L-alanyl-L-tryptophyl-D-phenylalanyl-L-lysinamide, maps residue-for-residue onto that sequence.2 The single feature that separates it from GHRP-6 is the 2-methyl group on the tryptophan at position 2, a substitution introduced in the original characterization work specifically to improve chemical stability over the parent peptide.1
That family lineage matters. GHRP-6 and GHRP-2 are the older parent peptides; hexarelin is the 2-Me-Trp-stabilized descendant.3 Ipamorelin, which people often lump into the same conversation, is a separate and later development — a more selective GHS-R1a agonist with less ACTH, cortisol and prolactin cross-activation — and it is not part of the CD36 cardiac literature described here. The cardiac side-story is specific to hexarelin and the classic GHRPs, not to ipamorelin.
How does the growth-hormone arm work?
The primary, best-documented action is GH release at the GHS-R1a receptor — the ghrelin receptor — expressed in the pituitary and hypothalamus.3 In the original Deghenghi characterization, hexarelin drove potent GH release in both infant and adult rats.1 The definitive human work came the same year: Ghigo and colleagues showed hexarelin stimulated GH secretion in humans after intravenous, subcutaneous, intranasal and — notably — oral administration, establishing it as an orally active secretagogue.4 A separate human dose-response study reported reproducible, dose-related GH release, corroborating the secretagogue arm independently.5
4 routes of administration — IV, subcutaneous, intranasal and oral — all produced GH release in the original human study.
Human desensitization is not the simple story the internet sometimes tells. Two human studies found that short-term intranasal or oral hexarelin did not blunt subsequent GH responsiveness — one in aging subjects,6 one showing no desensitization to later GHRH-mediated GH secretion in patients with anorexia nervosa.7 Continuous or high-frequency exposure can attenuate GH output, so the honest reading is that the effect is route- and schedule-dependent, not a fixed property of the molecule.
What is the CD36 cardiac side-story?
Here the pharmacology forks. When researchers tracked where hexarelin binds in the heart, the cardiac binding protein purified from rat cardiac membranes turned out to be CD36 — a scavenger receptor — not GHS-R1a.8 In that anchor study by Bodart and colleagues, the coronary vasoconstrictor response to the peptide was absent in CD36-null mouse hearts and in CD36-deficient spontaneously hypertensive rat (SHR) hearts, pinning the cardiovascular action on CD36.8 Worth stating plainly: the response measured there was vasoconstriction, an increase in coronary perfusion pressure. The CD36 axis is a mechanism of interest, not a uniformly “protective” one.
The heart binds hexarelin through CD36, a scavenger receptor — a target with no direct role in growth-hormone release.
The GH-independence was shown directly. Locatelli and colleagues reported that hexarelin protected the hearts of hypophysectomized rats — animals with GH signaling surgically removed — from ischemia-reperfusion damage, while a GHRP that does not bind the heart (EP 51389) was ineffective.9 Later work reinforced the same theme from different angles: hexarelin improved post-myocardial-infarction outcomes even in ghrelin-knockout mice,10 and a single oral dose preserved chronic cardiac function after infarction in rodents.11 Chronic administration also reduced cardiac fibrosis in SHR rats.12
The CD36 story is not confined to the heart. The same dual GHS-R1a/CD36 binding drives PPARγ-dependent cholesterol efflux and sterol-transporter upregulation in macrophages,13 and promotes mitochondrial biogenesis in white adipocytes.14 That is a broad metabolic pathway, distinct from GH release and consistent across tissues.
| Axis | Receptor | Reported effect (model) | Species / setting |
|---|---|---|---|
| GH release | GHS-R1a (ghrelin receptor) | GH secretion, multiple routes | Rats; humans |
| Cardiac binding | CD36 (scavenger receptor) | Coronary response; ischemia-reperfusion protection | Rat / mouse hearts, ex vivo |
| Metabolic | CD36 / GHS-R1a | Cholesterol efflux; mitochondrial biogenesis | Macrophages; adipocytes (in vitro / rodent) |
All cardiac and metabolic entries are rodent, ex-vivo or in-vitro findings. None represents a demonstrated effect in humans or a use recommendation of any kind.
An honest read of the evidence
The GH-secretagogue arm is solid and human-tested. The cardiac arm is where care is needed. It is overwhelmingly rodent and ex-vivo perfused-heart data; there are no controlled human trials of hexarelin as a cardioprotective agent. Human data are limited to short GH-secretagogue and pituitary-reserve testing — the endocrine work, not the cardiology.
Replication is also thinner than the volume of papers suggests. Several pivotal cardiac studies cluster around a small number of collaborating groups — the Ong and Bodart work in Montreal for CD36, the Milan Locatelli and Deghenghi group for cardioprotection, and the Kangawa group for post-infarction models. Independent, large-scale replication of the cardioprotection claims is limited. There is a specific methodological wrinkle worth flagging: some remodeling and fibrosis work uses spontaneously hypertensive rats, a strain that is itself CD36-deficient, which complicates any clean attribution of those effects to CD36 signaling. And the CD36 activation seen by Bodart produced coronary vasoconstriction, so “CD36 axis” and “cardioprotection” are not interchangeable — the cardiovascular effects are context-dependent, not a simple benefit narrative. Desensitization is likewise mixed: the human negatives are short-term and low-frequency, and should not be over-read as “hexarelin never desensitizes.” No safety or toxicology package supports human use, and much of the popular framing online extrapolates well beyond this mostly preclinical base.
All materials supplied by Condor Research are Research Use Only (RUO). Everything above reflects in-vitro and literature findings and is not a dosing protocol, clinical guidance, or a safety assessment for any organism. Hexarelin holds no marketing authorization as a medicine from the EMA or FDA and is a WADA-prohibited substance in the growth-hormone-secretagogue class; it is not for human or animal administration.
Condor Research · Wetenschappelijke helpdesk
Atrio Sciences s.r.o., IČO 57 669 651, Nitra (SK) · info@condorresearch.com
- Hexarelin (INN examorelin; CAS 140703-51-1; C47H58N12O6; MW ~887) is a six-residue GH secretagogue whose defining feature is a 2-methyl-Trp substitution at position 2, added to GHRP-6's scaffold for chemical stability.
- Its GH-releasing action runs through the GHS-R1a ghrelin receptor in the pituitary and hypothalamus; GH release was documented in humans across IV, subcutaneous, intranasal and oral routes.
- The distinctive cardiac binding target in rat heart was purified and identified as CD36, a scavenger receptor — not GHS-R1a; the coronary response was absent in CD36-null and CD36-deficient hearts.
- Cardioprotective effects in rodents were GH-independent: hexarelin protected hearts of hypophysectomized rats from ischemia-reperfusion, where GH signaling is removed.
- The same CD36 axis drives PPARγ-dependent cholesterol efflux in macrophages and mitochondrial biogenesis in adipocytes — a metabolic pathway distinct from GH release.
- The cardiac literature is overwhelmingly rodent and ex-vivo, clusters around a few collaborating labs, and includes CD36-mediated coronary vasoconstriction — so the axis is a mechanism of interest, not a proven therapy.
- Hexarelin has no marketing authorization as a medicine and is a WADA-prohibited substance; it is handled strictly as Research Use Only.
Is hexarelin the same as GHRP-6?
No. Hexarelin is a stabilized analog of GHRP-6, produced by substituting a 2-methyl-tryptophan at position 2 to improve chemical stability. GHRP-6 and GHRP-2 are the older parent peptides in the same family.
Does hexarelin act through the ghrelin receptor?
Its GH-releasing arm does, acting at GHS-R1a in the pituitary and hypothalamus. Its cardiac binding, by contrast, was traced to a different receptor, the scavenger receptor CD36. The two arms are pharmacologically distinct.
Is the cardioprotection real in humans?
There are no controlled human cardioprotection trials. The cardiac findings are entirely rodent and ex-vivo perfused-heart data, and one of the CD36-mediated coronary responses was vasoconstriction rather than an unambiguous benefit. The literature describes a mechanism of interest, not an established therapy.
Does hexarelin cause desensitization?
The evidence is mixed and schedule-dependent. Short-term intranasal or oral hexarelin did not blunt subsequent GH responsiveness in two human studies, though continuous or high-frequency exposure can attenuate GH output. The honest framing is route- and schedule-dependent.
How is hexarelin different from ipamorelin?
Ipamorelin is a later, more selective GHS-R1a agonist with less ACTH, cortisol and prolactin cross-activation, and it is not part of the CD36 cardiac literature. That cardiac story is specific to hexarelin and the classic GHRPs. For background on the wider class, see our overview of growth hormone secretagogues and the guides to GHRP-6, GHRP-2 and ipamorelin.
Is hexarelin an approved medicine?
No. It is an investigational peptide with no marketing authorization from the EMA or FDA and is prohibited in sport as a growth-hormone secretagogue. Condor Research handles it strictly as Research Use Only, not for human or animal administration.